
















 59 / 536
59 / 536

the public, especially in educational establishments and
health and social institutions, due to the risk of lung cancer
attributable to prolonged exposure to radon. Since August
2008, this compulsory monitoring has been extended
to workplaces located in priority geographical areas.
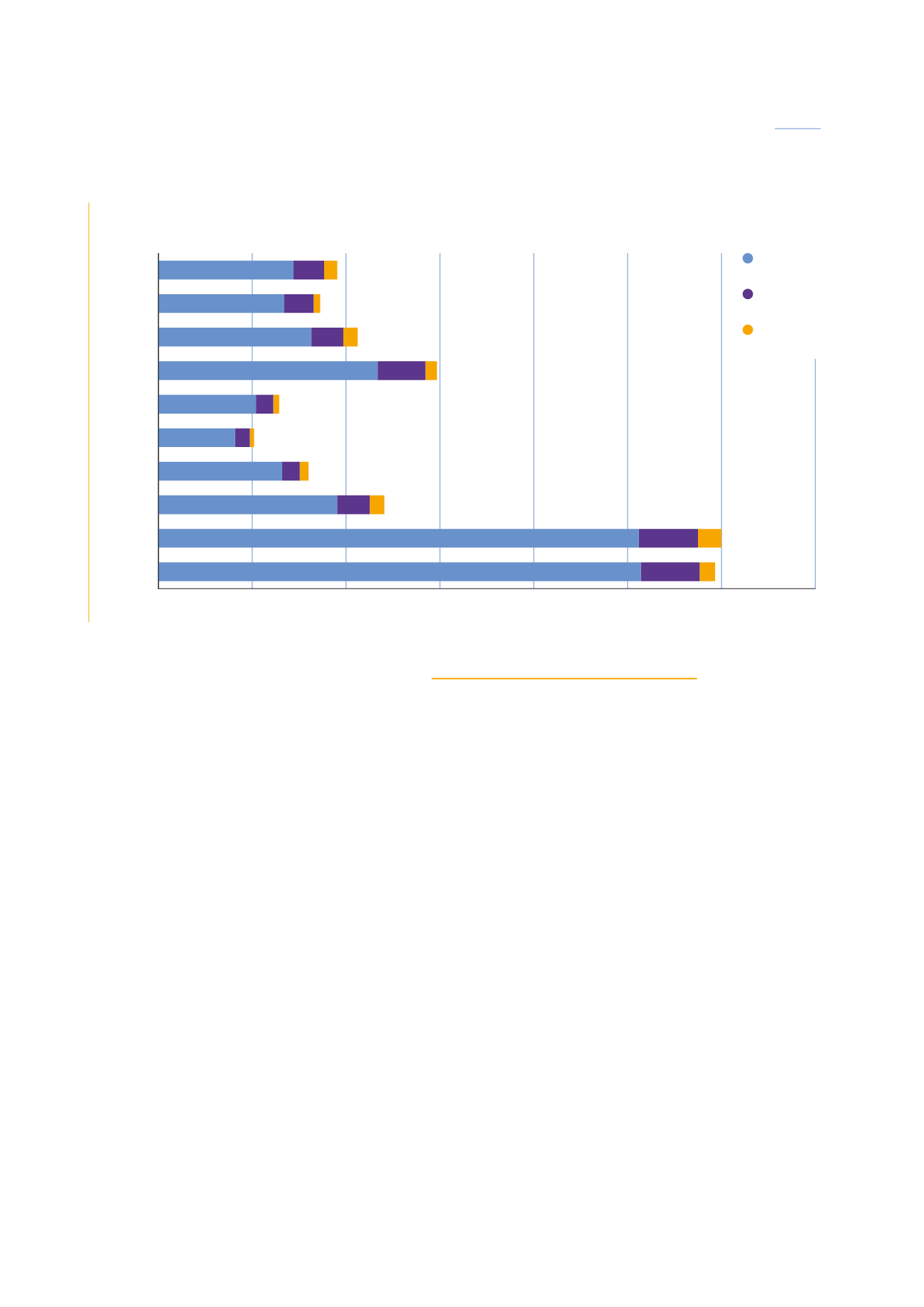
Results of the measurement campaigns conducted since
2005 by organisations approved by ASN are presented in
diagram 4. The percentages of the measurement results
that exceed the action levels (400 and 1,000 Bq/m
3
)
remain comparable from one year to the next. A new
ten-yearly screening cycle was started in 2009.
The results of the inspections in places open to the public
are not appropriate for precisely assessing the doses linked
to exposure of the general public due to the fact that
exposure in the home accounts for the largest part of the
doses received during one’s lifetime. It should be noted
that the data for the average activity concentrations of
radon in the home date from the national radon exposure
measurement campaign carriedout in the years 1980-1990.
Over and beyond the regulatory aspects (see chapter 3),
the management of radon risks formed the subject
of an interministerial action plan for the period
2011-2015, coordinated by ASN. The results of this plan
and the new action plan will be published in 2016 for
the 2016-2019 period.
3.3 Doses received by patients
In France, exposure for medical purposes represents
the greatest part of the artificial exposures of the public
to ionising radiation. This medical exposure has been
increasing over the last thirty years or so due to the rise in
the number of radiological examinations – and computed
tomography examinations in particular, to the ageing
of the population, and to the strategies implemented to
ensure better patient care, particularly in the context of
patient monitoring after cancer treatment and coronary
diseases. It has been regularly reviewedby IRSNsince 2002.
The average effective dose per inhabitant resulting
from diagnostic radiological examinations has been
evaluated at 1.6 mSv for the year 2012 (IRSN report
2014) for some 81.8 million diagnostic procedures
performed (74.6million in 2007), i.e. 1,247 procedures
for 1,000 inhabitants per year. It is to be noted that
the individual exposure in 2012 is very varied. Thus,
although about one third of the French population
underwent at least one procedure (excluding dental
procedures), 85% of that population was not exposed
or received doses of less than 1 mSv.
The average effective individual dose increased by 23%
between 2007 and 2012 (it was 1.3mSv in 2007); it had
already increased by 50%between 2002 and 2007 (IRSN/
InVS report 2010). It must nevertheless be underlined
that the methodologies used for the 2002-2007 period
and the 2007-2012 period were not identical.
DIAGRAM 4:
Results of radon measurement campaigns
0
500
1,000
1,500
2,000
2,500
3,000
3,500
2012/2013
2013/2014
2014/2015
815
671
156
35
76%
78%
18% 4%
720
163
70
75.55%
17.10% 7.35%
1,168
79%
255
17%
170
16%
77
7%
61
4%
520
81%
92
14%
32
5%
659
82%
94
12%
47
6%
952
79%
2,560
85%
174
15%
78
6%
315
11%
125
4%
87%
10%
3%
409
80%
78
15%
23
5%
2011/2012
2010/2011
2009/2010
2008/2009
2007/2008
2006/2007
2,570
314
82
2005/2006
Measurement campaign
Number and percentage of checked establishments
Source: IRSN.
Etablishments at higher
than 1,000 Bq/m
3
Etablishments between
400 Bq/m
3
and 1,000 Bq/m
3
Etablishments at less than
400 Bq/m
3
59
CHAPTER 01:
NUCLEAR ACTIVITIES: IONISING RADIATION AND HEALTH AND ENVIRONMENTAL RISKS
ASN report on the state of nuclear safety and radiation protection in France in 2015